Fidelity in mental health services: Clinical strategies for implementing resource groups
Main Article Content
We investigated whether or not people working in the fields of psychiatry and social work who do not have experience in assessing the fidelity of resource group assertive community treatment could use a new manual for the Clinical Strategies Implementation Scale–Revised (CSI–R) in a reliable and valid fashion. Participants were 4 men and 17 women who were caregivers recruited from psychiatric and social-work clinics in Middle Sweden. The study was conducted using a combination of quantitative and qualitative techniques. The caregivers were asked to rate 2 fictional cases individually and thereafter discuss their assessments in focus groups. Results indicated acceptable values for homogeneity, criterion validity, and divergent validity. We concluded that people working in the fields of psychiatry and social work who are inexperienced in using the CSI-R can use it in a reliable and valid way with the help of the new manual, and that the procedure used to conduct the study can be used as a model for a brief educational program or seminar.
Within treatment effectiveness research, fidelity is currently considered a component of the assessment process routinely used to ensure internal validity (Hohmann & Shear, 2002). Assessments of fidelity are also of importance in that they provide a foundation for making evaluations of whether unsuccessful outcomes are caused by a failure of the model or failure in correctly implementing the model, that is, in the process of transferring the model to the clinical setting (Chen, 1990). Fidelity has been defined as “the extent to which delivery of an intervention adheres to the protocol or program model originally developed” (Mowbray, Holter, Teague, & Bybee, 2003, p. 315).
Assertive community treatment (ACT) is a societally based treatment and rehabilitation program that was developed during the 1970s and 1980s in the USA. The program was primarily geared to treatment of people with chronic psychiatric illnesses who were in need of a great deal of inpatient care (Stein, 1990; Stein & Santos, 1998; Test & Stein, 1978). In its original form, ACT consisted of psychiatric-care teams in which all the members would work with all the clients and all the members had a case management function (Lewin Group, 2000). It was clearly outlined how many staff members there ought to be in those teams, what their function was, and which treatment techniques were to be used in the environment of the clients. Given that background, it gradually became clear that a reliable and valid instrument to assess the fidelity of the application of ACT should be developed. Such an instrument became available in the Dartmouth Assertive Community Treatment Scale (DACTS), which soon became the standard fidelity measure for ACT and undoubtedly contributed to improvements in regard to the implementation and application of the model (Bond & Salyers, 2004; Monroe-DeVita, Teague, & Moser, 2011; Teague, Bond, & Drake, 1998).
The DACTS, however, is not suited for use with all models and especially not for use with a model such as the resource group assertive community treatment (RACT; Falloon, 1999), which has as a starting point working with a network of clients with the help of a small but flexible team (Nordén, Eriksson, Kjellgren, & Norlander, 2012; Nordén, Ivarsson, Malm, & Norlander, 2011; Nordén, Malm, & Norlander, 2012). The construct of fidelity within the model was at first examined in accordance with a heuristic model in which the fidelity of the program was primarily controlled with the aid of different systems of results follow-up (Falloon et al., 1997). However, the need for a fidelity instrument was significant and, on the basis of experience, an instrument especially adjusted for work with resource groups was eventually constructed, namely the Clinical Strategies Implementation Scale (CSI; Falloon et al., 2005). With time, however, it was shown that the instrument needed further adjustments for use when working with resource groups, and the psychometric characteristics needed strengthening. A revision of the scale was commissioned by the Quality Star National Psychiatric Register in Sweden. The revised version (CSI–R) exhibited good psychometric characteristics (Andersson, Ivarsson, Tungström, Malm, & Norlander, 2014).
Staff in clinical psychiatric operations associated with the Quality Star National Psychiatric Register put forward a request for a manual for the CSI–R in order that even inexperienced raters might use the instrument in a reliable and valid fashion. An editorial committee was formed whose members began the process by analyzing how experienced raters used the instrument. On the basis of this analysis the topics of each of the nine items of the CSI–R were divided into components. Thereafter, the committee defined how many of the various components of each item should have been included in each step of the scale and it was then possible to decide the assignment of points to the five steps for a certain scale item as follows: scale point 0 = none or very few components executed; scale point 1 = two components executed; scale point 2 = in the work with the client three components have been executed; scale point 3 = all four components have been executed several times. It is assumed that the resource group meets on a regular basis; scale point 4 = all four components executed several times and applicable elements of the RACT manual have been considered and been used by the client on his/her own. It is assumed that the resource group meets on a regular basis.
Purpose and Research Questions
Our purpose with this study was to examine how people working in the fields of psychiatry and social work who have had no practical experience with either the CSI or the CSI–R perceive the instrument in regard to using a new instruction manual. Given that background, we formulated three research questions: (a) Can the resource group staff use the CSI–R in a reliable and valid fashion with the manual as a starting point? (b) Are there differences between those working in psychiatry and those working in social work with regard to their perception of the manual and a subsequent discussion of calibration? (c) Is the procedure used to conduct the study a suitable model for a brief but effective educational program in teaching how to use the CSI–R and the instruction manual for use of the instrument?
Method
Participants
The participants were 21 caregivers (4 men and 17 women) with a mean age of 49.38 years (SD = 11.48, range = 27 to 64 years) who were recruited within psychiatry and social work services in seven towns of Middle Sweden. Their occupations were care attendants (16 people), case managers (3 people), and nurses (2 people). Ten of the participants were employed by the regional psychiatry services and 11 were employed by the local social services provider. With only one exception the participants had received special training in use of RACT, either as a brief training of eight days over a six-month period (seven individuals) or as a more comprehensive course based on 48 days over a period of two years (13 individuals). When we conducted the current study it was two or three years since the participants had completed these training sessions. After they finished the RACT training, 14 of the participants had attended meetings of resource groups with one of their clients and had run these meetings on one or several occasions with their client. The seven other participants had only had sporadic experience with resource group work since completing their RACT training.
Design
We used a combination of quantitative and qualitative techniques in the study. Quantitative data were collected by way of a survey (background data, test sheets for assessments of the CSI–R and the understanding of the manual, and discussions in focus groups) and qualitative data were collected through recorded discussions within five focus groups. A prerequisite for participation was that the caregivers had experience with psychiatric or social work and that they had at least vague knowledge of the RACT model, but no experience, or minimal experience, of having completed the CSI or CSI–R. A control of experience was obtained by having the participants respond to two visual analogue scales (VAS) ranging from 0 to 100. On the question regarding whether or not they had had a great deal of experience of doing self-assessments with the instrument, a mean of 13.90 (SD = 1.48) was obtained, and on the question on whether or not they had had a great deal of experience being rated by an external expert with the instrument, a mean of 14.71 (SD = 0.73) was obtained.
Every participant was given the assignment of rating from a detailed description, one case that, according to the CSI–R, would yield a relatively low fidelity score, and a second case that would yield a relatively high fidelity score on the CSI–R. A highly skilled instructor and educator working with the RACT method composed the description of the two cases, with the low-fidelity case corresponding to approximately 35 points on the CSI–R, and the high-fidelity case corresponding to approximately 85 points. Those levels were blindly corroborated by a second highly skilled instructor. In order that gender stereotypes would not play a role in the ratings, two of the groups (10 participants) were given the case with the low fidelity with a male name, and the case with high fidelity with a female name, whereas three of the groups (11 participants) were given a female name for the case with a low fidelity, and a male name for the high-fidelity case. In order to avoid presentation-order effects, two of the groups (seven participants) started with the case with low fidelity, and three of the groups (14 participants) started out with the case with high fidelity.
Instruments
Background data. Participants completed a questionnaire in which they provided demographic data on gender, age, employment (regional psychiatry or local social-care institution), professional affiliation, as well as what training they had received on the RACT model. In addition, the participants indicated the extent to which they had previous experience of working with resource groups, how often they had done self-ratings with the CSI–R, and finally whether or not they had ever been evaluated by an external expert on the CSI–R.
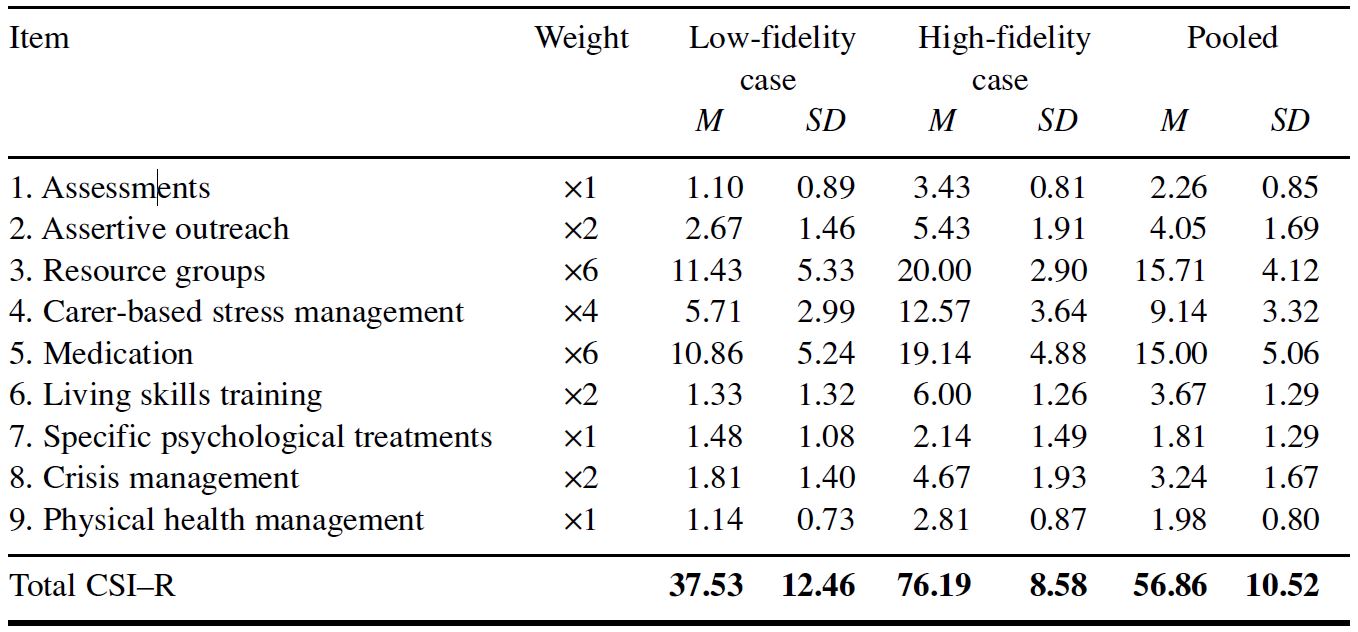
Clinical Strategies Implementation Scale–Revised (CSI-R). The CSI–R (Andersson et al., 2014) consists of nine ordinal scales devised to measure key aspects of treatment strategies that have been associated with clinical and social recovery within the framework of the RACT. The scales range from 0 (none or only a few components executed) to 4 (all components executed) with the goal of covering nine domains. The nine domains are: (a) assessments, goals, and plans; (b) assertive outreach in society; (c) resource groups; (d) carer-based stress management; (e) medication; (f) living-skills training; (g) specific psychological treatments; (h) crisis management; and (i) physical health management. The various domains are weighted in accordance with their importance (see Table 1). This procedure yields a maximum score for the CSI–R of 100. The instrument includes a special protocol for rating of fidelity, executed in connection with each respective weighting. The instrument has been shown to have good psychometric characteristics (Andersson et al., 2014).
Manual for the Clinical Strategies Implementation Scale Revised. In order to facilitate the use of the CSI–R for inexperienced raters the members of the Quality Star National Psychiatric Register decided to construct a comprehensive manual designed to describe and discuss the various factors to which raters should pay attention. The Executive Committee of the Quality Star National Psychiatric Register then commissioned an editorial committee to compile an outline of a manual, the characteristics of which could then be tested in a study. In the manual that was produced, each domain is divided into several components as described earlier in this article.
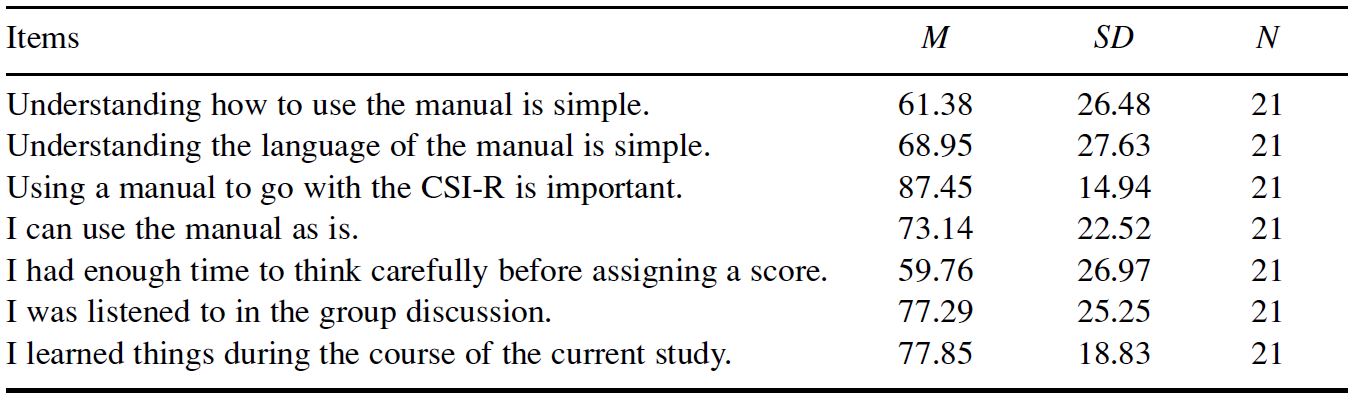
Concluding survey. After the focus discussions were concluded the participants completed a survey in which they indicated their views about the manual on seven VAS ranging from 0 to 100, with anchor points of do not agree at all to agree completely (see Table 2). In addition, there was room for additional comments.
Procedure
We contacted ten heads of operations within social services and psychiatric care asking them to allow their staff to participate in a study about whether or not individuals inexperienced with using the CSI–R would be able to complete the scale with the aid of a recently compiled manual. We also told the ten heads that a prerequisite for participation of their staff was that it would be completely voluntary. Heads of seven operations in towns with different geographical locations in Middle Sweden accepted, and thereafter written information about the study was sent to the staff members. The recipients of this information were told that participation was completely voluntary, and that anyone could stop taking part without having to give a reason. In response to the information pack, 21 caregivers signed up as participants in the study, yielding the possibility of forming five focus groups with a minimum of three members and a maximum of six members.
The same person moderated all five focus groups. At the sessions the original Swedish version of CSI–R was used and the Swedish language was also used when the participants completed the study instruments. The first of the focus group meetings began by the moderator first distributing a consent form that the participants read and signed. Thereafter the moderator handed out the newly compiled manual. The participants studied it individually for 10 minutes. The next step was for the moderator to hand out a written description of the first fictitious patient case in accordance with the previously arranged order (see the Design section) as well as the CSI–R protocol for the rating of the fidelity of the protocol. The participants were then given 20 minutes to individually rate the degree of fidelity in terms of the nine scales of the CSI–R. Thereafter the moderator collected the completed ratings. After this was done the moderator distributed a written description of the second fictitious patient case. Once again the participants had 20 minutes to rate the fidelity in terms of the CSI–R.
Following the collection of the ratings, and after a brief break, the group assembled in order to discuss both cases. The moderator made clear that the discussions would deal only with the two fictitious cases and actual patients of the caregivers would not be discussed. The discussions were recorded for the purpose of subsequent analysis. On average the participants needed 16.76 minutes (SD = 3.92) to discuss one case. The moderator did not have a ready-made discussion guide but followed the principles of an unstructured discussion, and facilitated the session so that the participants could freely choose what to discuss. Each session began with the moderator asking “How did you feel about the case?” During the course of the discussion the moderator might ask questions for clarification (e.g., “Could you expand on that? What was missing?”), or in order to guide the discussion to some topic in need of illumination (e.g., “What kind of picture did you get of the resource group when you were reading the case?”) When the discussions of the two cases were over, the moderator distributed the concluding survey, which the participants completed individually. That completed the study and the moderator thanked everyone for their participation.
Ethical Considerations
The information about the study was distributed to the staff at the seven operations. The content was based on the principles of the Helsinki Declaration and made clear that participation was completely voluntary and that each individual had the right to discontinue participation without having to provide a reason, and the informed consent sheet that the participants signed confirmed that all data would be decoded and treated confidentially. An additional ethical consideration was that all discussions were to be based on two fictitious patient cases and there would be no examples taken from actual patient files in the study. The Ethical Committee at the Evidens University College examined and approved the study.
Results
The CSI–R Ratings of the Participants
Order and gender effects with regard to cases. Seven of the participants were included in groups that rated the case with low fidelity first and thereafter rated the case with high fidelity, and 14 participants were members of groups that rated the cases in the reverse order. The results of analysis using the Wilcoxon Signed Ranks Test, 5% level, show no significant effect for order of presentation of cases (p = .289). Additional analyses with the Mann-Whitney U Test, 5% level, yielded no significant effects for gender, based on whether the person in the case study was given a male or female name (ps > .05).
Gender, employment type, and training of the caregivers. Analyses using the Mann-Whitney U Test, 5% level, with the pooled (i.e., the averaged) results from the two rating occasions as the dependent variable yielded no significant differences with regard to the gender of the caregivers (p = .237), whether they were employed locally or regionally (p = .378), or whether they had participated in either the shorter or longer case management training (p = .183).
Level of fidelity. In order to examine how the participants rated the fictitious cases characterized by low or high fidelity, an analysis was performed using the Mann-Whitney U Test, 5% level, with the pooled results as the dependent variable and with the fidelity level of the case (low fidelity, high fidelity) as the independent variable. The result of the analysis shows that there was a significant difference (Z = 3.66, p < .001), in the participants’ rating of the two cases with the high-fidelity case receiving a higher rating compared to the case with low fidelity. Pearson’s r, 5% level, showed no significant correlation between the case with high fidelity and the case with low fidelity (r = .08, p = .741), indicating discriminant validity. Concerning criterion validity, the participants’ ratings indicated acceptable validity as compared to the criteria (low fidelity case = 35 points; high fidelity case = 85 points). Means and standard deviations for the cases with low and high fidelity and the pooled results from the two ratings are shown in Table 1.
Table 1. Means and Standard Deviations for Participants’ Assessment of CSI-R Items in Regard to Low- and High-Fidelity Cases and the Pooled Results From Percentage Scores for Both Assessments
Reliability. The homogeneity of the fidelity ratings of the participants was examined using Cronbach’s alpha and yielded a high value for the first rating occasion (a = .89), an acceptable value on the second occasion (a = .74), and an acceptable value for pooled results (a = .70). Subsequent interitem analyses with one or several items deleted did not show any improvements with regard to Cronbach’s alpha.
The ratings of the participants on the visual analogue scales. In order to examine whether or not there were any differences between locally employed (social service) and regionally employed (psychiatry) participants with regard to the use of the manual and/or the length of their training (shorter vs. longer), we performed a one-way Pillai’s MANOVA with the seven VAS about participants’ opinions as dependent variables and employment type (local, regional) as the independent variable. The analysis yielded no significant difference between those locally or regionally employed (Eta2 = 0.29, p = .670), a finding that was also supported by the univariate F tests (ps > .05). The means and standard deviations for the seven VAS are set out in Table 2.
Table 2. Means and Standard Deviations for Participants’ Assessment of the Manual and the Study Procedure
Verbal Analysis
The discussions following the rating session were recorded on tape and were transcribed. The result was 51 pages of transcription contained in 10 documents (two from each focus group), which was analyzed by way of phenomenological qualitative analysis (Ingvarsson, Nordén, & Norlander, 2014). About half of the discussion time was spent on talking about the choice of score for each domain and what differed and united the ratings. In addition, a few linguistic comments were offered and participants expressed views on the layout of the manual. The discussion sessions assumed the shape of a calibration in terms of making constructive comments and suggestions with the purpose of finding a joint view of how to consider various aspects. The participants felt that this aspect of the study was both interesting and educational. Occasionally, there were some unnecessary discussions until a participant realized that he or she had overlooked an instruction in the manual.
The participants also indicated repeatedly in the discussions that it is necessary to do evaluations and follow-ups of the various elements of the CSI-R, and that this notion is a central issue in considering the fidelity of the RACT. The participants identified clear differences between the two cases to be rated. With regard to the case with low fidelity, there appeared to be a lack of alliance, structure, and involvement by the case manager, whereas the participants judged the case with high fidelity to have a high level of structure, involvement, mobilization of the client, and high fidelity. They were not asked about high fidelity directly. One of our purposes was to develop an approach that could later be used to train caregiver staff to use the CSI–R as a fidelity instrument in the setting of their ongoing activities. The results of the qualitative analysis strongly indicate that the participants perceived the approach as both interesting and educational with standard comments such as: “It became clear, I could see in front of me, the two different clients I have been working with lately,” “Group discussions around the two cases were good,” “I see the importance of initiating ratings of the cases I am working with,” “Good discussions toward the end,” “Interesting approach which triggered deep thought and repetition [of the elements in the RACT method],” “Very good and interesting.”
Discussion
Our purpose was to examine how caregivers without any practical experience with either the CSI or the CSI-R feel about the instrument.
With regard to whether or not the resource group staff could use the CSI-R in a reliable and valid fashion, the Cronbach’s alpha shows an acceptable value for the pooled results from the two case ratings. The fact that the value on the first assessment was higher compared to that on the second assessment might be explained by the fact that 14 of the 21 participants were first presented with the case with high fidelity and that they might have been more in agreement in the assessment of that case, a notion also put forward by the participants in the subsequent discussions. Both criterion and divergent validity were examined. In terms of the criterion validity, the predicted outcome was to a high degree in accord with the participants’ ratings of the case with low fidelity, whereas their ratings for the case with high fidelity were somewhat below the predicted value. However, the participants’ ratings of the mean for the case with high fidelity was 76.19, which is above the critical value of 75, where previous experience has shown that the methods and strategies of RACT have been implemented and where the positive changes in the clients usually last over time (Nordén & Norlander, 2015). The assessment of divergent validity is used when it is expected that the two variables examined will be unrelated (Norlander, Bood, & Archer, 2002; Wilson, Gullone, & Moss, 1998). The analyses of the cases with low and high fidelity show a significant difference between the ratings, and Pearson’s r was at the level of zero. In addition, the participants’ verbal analyses confirm that they perceived several significant types of differences between the two cases.
We examined possible differences between those employed within psychiatry and within social work in how they perceived the manual and the subsequent discussion. The results of analysis show that there was no difference between those employed within psychiatry and those employed within social work in how they responded to the VAS. This finding is important because collaboration between these two professional groups is essential for optimal functioning of the work with resource groups in the network of clients. Against the background that the participants had not previously seen the manual, they assigned surprisingly high scores with regard to their understanding of the language used in the manual and about its use. The participants perceived it as important to use a manual in connection with the CSI–R and also that the manual in its current form was fit for purpose. In terms of the subsequent discussions, the participants’ ratings of these, as well as their verbal analyses, indicate that several of them felt it was stressful to find the time to think through the case before assigning the score. On the other hand, a majority felt that they were given the time to speak during the focus discussions and that they learned new things throughout the study.
Finally we examined whether or not the study method and procedure might function as an educational program for staff within psychiatry and social work in how to use the CSI–R. It had already became evident in connection with our examination of the use and usefulness of the manual that the participants felt that they learned new things throughout the study. This result is in line with the focus discussions, where there was almost total concordance of all participants in the view that the study was both interesting and educational.
The evaluation of the psychometric characteristics of the manual was further strengthened by the statistical controls that show that it made no difference whether the cases were presented with the high-fidelity case first or the low-fidelity case first, and this was also true for whether the case was presented with a male or a female name. Additional analyses show that the gender of the participants, their professional status, or academic qualifications also did not make any difference to how the participants rated the degree of fidelity. A deficit in the study was, however, that the participants did not have the opportunity to do yet another rating of a fictitious case following the discussions. The inclusion of such a procedure would have provided evidence about whether or not the participants had become even more concordant as a result of taking part in the focus discussions.
We concluded, however, that the results we obtained in the study show that the compilation of the manual has contributed to the capacity of inexperienced raters within psychiatry and social work to use the CSI–R in a reliable and valid way and that the procedure we used to conduct the study can be used as a model for a brief educational program or seminar.
Andersson, J., Ivarsson, B., Tungström, S., Malm, U., & Norlander, T. (2014). The Clinical Strategies Implementation Scale Revised (CSI-R). Fidelity assessment of Resource Group Assertive Community Treatment. Open Journal of Medical Psychology, 3, 36–41. http://doi.org/9th
Bond, G. R., & Salyers, M. P. (2004). Prediction of outcome from the Dartmouth Assertive Community Treatment Fidelity Scale. CNS Spectrums, 9, 937–942.
Chen, H. (1990). Theory-driven evaluations. Thousand Oaks, CA: Sage.
Falloon, I. R. H. (1999). Rehab rounds: Optimal treatment for psychosis in an international multisite demonstration project. Psychiatric Services, 50, 615–618. http://doi.org/bffq
Falloon, I. R. H., Economou, M., Palli, A., Malm, U., Mizuno, M., Murakami, M., & Optimal Treatment Project Collaborative Group. (2005). The Clinical Strategies Implementation Scale to measure implementation of treatment in mental health services. Psychiatric Services, 56, 1584–1590. http://doi.org/cm6zfr
Falloon, I., Fadden, G., Borell, P., Kärräng, L., Ivarsson, B., & Malm, U. (1997). Integrerad psykiatri
[Integrated psychiatry]. Värnamo, Sweden: Psykologia.
Hohmann, A. A., & Shear, M. K. (2002). Community-based intervention research: Coping with the “noise” of real life in study design. The American Journal of Psychiatry, 159, 201–207. http://doi.org/ctptxg
Ingvarsson, T., Nordén, T., & Norlander, T. (2014). Mindfulness-based cognitive therapy: A case study on experiences of healthy behaviors by clients in psychiatric care. Open Journal of Medical Psychology, 3, 390–402. http://doi.org/9v6
Lewin Group. (2000). Assertive community treatment literature review. Prepared for health care and financing administration and substance abuse and mental health services administration. Falls Church, VA: The Lewin Group.
Monroe-DeVita, M., Teague, G. B., & Moser, L. L. (2011). The TMACT: A new tool for measuring fidelity to Assertive Community Treatment. Journal of the American Psychiatric Nurses Association, 17, 17–29. http://doi.org/dcz4v3
Mowbray, C. T., Holter, M. C., Teague, G. B., & Bybee, D. (2003). Fidelity criteria: Development, measurement, and validation. American Journal of Evaluation, 24, 315–340. http://doi.org/bnmjrf
Nordén, T., Eriksson, A., Kjellgren, A., & Norlander, T. (2012). Involving clients and their relatives and friends in psychiatric care: Case managers’ experiences of training in resource group assertive community treatment. PsyCh Journal, 1, 15–27. http://doi.org/f234h9
Nordén, T., Ivarsson, B., Malm, U., & Norlander, T. (2011). Gender and treatment comparisons in a cohort of patients with psychiatric diagnoses. Social Behavior and Personality: An international journal, 39, 1073–1086. http://doi.org/d8rqqb
Nordén, T., Malm, U., & Norlander, T. (2012). Resource Group Assertive Community Treatment (RACT) as a tool of empowerment for clients with severe mental illness: A meta-analysis. Clinical Practice & Epidemiology in Mental Health, 8, 144–151. http://doi.org/f24vwm
Nordén, T., & Norlander, T. (Eds.). (2015). Resursgrupps ACT (RACT) – en flexibel och integrativ metod [Resource Group ACT (RACT) – a flexible and integrative method]. Gothenburg, Sweden: Evidens University Press.
Norlander, T., Bood, S. Å., & Archer, T. (2002). Performance during stress by different occupational groups: Affective personality, age, and regularity of physical exercise. Social Behavior and Personality: An international journal, 30, 495–508. http://doi.org/b7jz8p
Stein, L. I. (1990). Comments made by Leonard Stein. Psychiatric Services, 41, 649–651. http://doi.org/bffp
Stein, L. I., & Santos, A. B. (1998). Assertive Community Treatment of persons with severe mental illness. New York, NY: Guilford Press.
Teague, G. B., Bond, G. R., & Drake, R. E. (1998). Program fidelity in assertive community treatment: Development and use of a measure. American Journal of Orthopsychiatry, 68, 216–232. http://doi.org/crz3hs
Test, M. A., & Stein, L. L. (Eds.). (1978). Alternatives to mental hospital treatment. New York, NY: Plenum Press.
Wilson, K., Gullone, E., & Moss, S. (1998). The youth version of the Positive and Negative Affect Schedule: A psychometric validation. Behaviour Change, 15, 187–193.
Table 1. Means and Standard Deviations for Participants’ Assessment of CSI-R Items in Regard to Low- and High-Fidelity Cases and the Pooled Results From Percentage Scores for Both Assessments
Table 2. Means and Standard Deviations for Participants’ Assessment of the Manual and the Study Procedure
The Clinical Strategies Implementation Scale with its accompanying manual has been revised (CSI-R) in a collaboration of the Evidens University College
Gö
teborg
Sweden
Quality Star National Psychiatric Register
Kungä
lv
and the Optimal Treatment Project Practice Foundation. Jonny Andersson
Bo Ivarsson
and Ulf Malm were members of the editorial committee who wrote the manual the use of which was examined in the current study.
The authors wish to thank the psychiatric outpatient clinics of Arvika
Karlstad
Mora
and the psychiatric clinic at the Falkö
ping Hospital
as well as the social work services in Arvika
Forshaga
Kristinehamn
and Rä
ttvik.
Torsten Norlander, Center for Research and Development, Evidens University College, Packhusplatsen 2, SE-411 13 Göteborg, Sweden. Email: [email protected] or [email protected]