Gender and treatment comparisons in a cohort of patients with psychiatric disorders
Main Article Content
Our purpose in this study was to make group comparisons of the Swedish psychiatric patient cohort called Quality Star. The present study included 1,376 patients, 753 men and 623 women, recruited from 9 outpatient clinics over the space of 6 years. All participants had serious mental illnesses, of which patients with a schizophrenia spectrum disorder were the majority. The 4 aspects studied were consumer satisfaction, life quality, social function, and symptoms. The study had 2 main outcomes: (a) women were more satisfied with the health care and had better functioning than men, (b) patients treated according to the Integrated Care Program had better functioning and less severe symptoms than other patients. The differences between diagnosis groups were as expected.
In 2000, after some development work, a network was established between primarily psychiatrists and other caregivers in clinical practice in western Sweden with the purpose of using a method named Quality Star [in Swedish: Kvalitetsstjärnan] (Erdner & Ivarsson, 2001; Ivarsson, Erdner, & Malm, 2006). The purpose of Quality Star was to provide psychiatry with easy, nationally applicable outcome measures in order to give a brief overview of the patient’s situation and to describe the effects of treatment in relation to factors of relevance, related to both patient and medical care, for the treatment results.
Throughout the years, the network has, to a certain limited extent, been used to make some compilations in order to confirm the psychometric and statistical properties of the instruments (e.g., Erdner & Eiman, 2003; Thörnborg, Nordholm, Wallström, & Svantesson, 2005). Over time, the amount of collected data grew and is now considered sufficient for conducting in-depth research with a higher degree of accuracy. It was recently decided that a vast research program in two steps is to be carried out. Step One includes analyzing the material collected during the first 10 years with the purpose of (a) assessing the psychometric properties of Quality Star and (b) investigating group differences within the cohort between patients with different background characteristics and with different intervention patterns.
Step Two involves investigating how newly added clinics, in collaboration with already established care units, implement their work with Quality Star and new methods of treatment, especially the integrated care program, which during the past few years has made great advances in Sweden (Burns & Firn, 2002; Malm, 2002). The integrated care program method was developed through an international research project called the optimal treatment project (Falloon, 1999), an ongoing program which started in 1994. The treatment program as a whole has been scientifically tested in a number of different countries with various types of health care and welfare systems. In the program, it was found that the program is most effective if participants themselves set the goals for their treatment and have a decisive impact on how it is to be designed.
Quality Star is a measurement system encompassing eight dimensions (consumer satisfaction, quality of life, psychosocial functioning, burden for important other, resource dimension, group specific dimension, symptom severity, subjective distress). For each dimension there are tests that are summed up on a scale ranging from 0–100, where 0 means very ill and 100 means they are as healthy as can be. Patients rate their consumer satisfaction, quality of life, and subjective distress; their next of kin rate perceived burden; and health care staff rate the other dimensions. By presenting the star as a figure resembling a sun with eight rays, a graphic picture of the patient’s situation is displayed by linking together the points on the different rays. The further out on the rays that the points are scored, the healthier the patient is. Hence, the patients, their next of kin, and the care staff are provided with a synoptic figure on which the effects of interventions can be studied. The eight dimensions can be viewed in Figure 1. Apart from these core variables, data are also collected regarding diagnosis, age, gender, illness duration, contact duration with health care, caregivers, and a brief outline of the health care intervention.
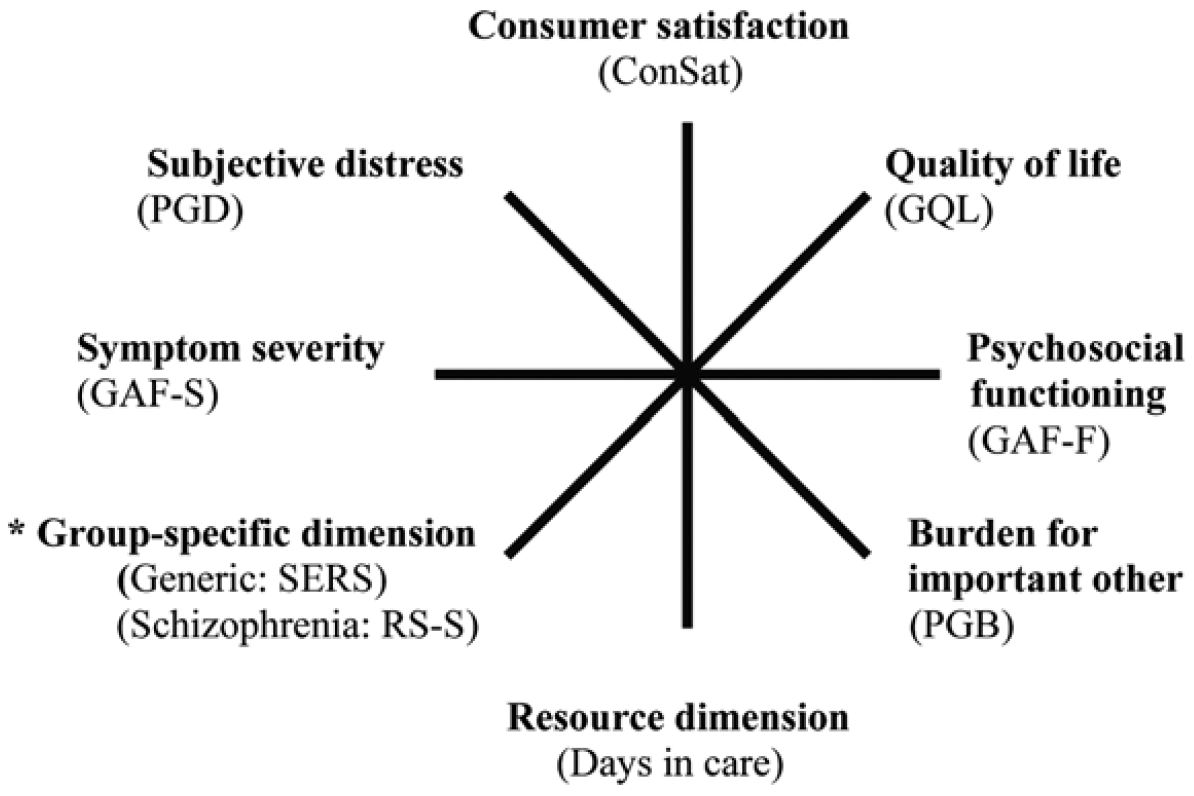
Figure 1. Graphic presentation of the Quality Star. The recognized abbreviations of the instruments are presented in parentheses. (Taken from Ivarsson, Malm, Lindström, & Norlander, 2010.)
* This axis is intended for group-specific extra measures when suitable. Health screening (SERS) in general is recommended. For psychosis groups, Remission index (RS-S) is now being introduced.
This study is the first in a series aimed at investigating the differences and similarities between the various patient groups included in the clinical cohort examined with the different instruments that make up the Quality Star test battery. In this study we focus on analyzing two of the dimensions where the patients rate themselves; namely, satisfaction with health care regarding treatment and intervention (consumer satisfaction) and subjectively experienced quality of life. Additionally, two of the dimensions rated by caregivers are analyzed, i.e., function and symptom. Data were collected during 2003-2008 and analyzed in three two-year periods in order to allow for taking possible changes across time into consideration
The aim in this study was to investigate differences on a group level between patients with various background characteristics by scrutinizing four of Quality Star’s eight dimensions. Considering clinical experience (Andersson, 2008; Eiman & Ivarsson, 2009; Malmström, 2008) the following four questions were of particular interest to us: Are there differences that can be derived from the fact that data were collected at different intervals?; Are there differences between patients diagnosed within the schizophrenia spectrum, and patients with other psychiatric diagnoses?; Are there differences between men and women?; and, Are there differences between patients treated according to the Integrated Care Program, and patients who were treated using other methods?
Method
Participants
Participants were 1,376 patients: 753 men and 623 women. All had filled out the Quality Star questionnaire on at least one occasion at 1 of the 9 participating psychiatric centers during 2003-2008. No patient in this study had filled out the Quality Star questionnaire more than once during the same year. In total, 2,934 Quality Stars were collected during the 6-year period, which gives an average of 2.13 ratings for each patient (SD = 1.40, range = 1-6). The participants were a mix of patients who could all be defined according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994) as suffering from serious mental illnesses (SMI). The majority of patients were within the schizophrenia spectrum (82.8 %), while the other patients (17.2 %) had a variety of typical psychiatric diagnoses such as delusional syndrome, mental disturbances, addiction syndrome, bipolar disorder, depression, cyclothymic disorder, dysthymic disorder, panic disorder, anxiety disorders, obsessive-compulsive disorder, behavioral disorders, personality disorders, and attention disorders. The mean age of the patients was 50.15 years (SD = 12.81, range = 20–89). Of the 1,376 patients included in the study, 133 persons (66 men and 67 women) were recruited from the Lysekil Clinic, which was used for comparisons because the staff have worked with the Integrated Care Program method since 1994.
Instruments
Consumer Satisfaction Rating Scale (ConSat; Ahlfors et al., 2001; Ivarsson & Malm, 2007) This instrument is used to measure perceived level of satisfaction with the care given, and is based on 12 questions within eight different areas (availability, atmosphere, treatment modalities, information, drug treatment, psychosocial interventions, usefulness of treatment/care, and general well-being). Each question is answered on a 7-point scale with the anchor points not satisfied at all and completely satisfied. The total sums for the eight different areas are then transformed to a scale ranging from 0–100, where 0 indicates not satisfied at all and 100 indicates completely satisfied. Consumer satisfaction (ConSat) has shown good psychometric properties (Ivarsson & Malm, 2007). In Quality Star the first 11 items are used as the ConSat measure. The 12th (general well-being) coincides with the separately used quality of life axis, namely the GQL.
Global Quality of Life (GQL) The instrument (GGG-group, 2009; Thörnborg et al., 2005) was specifically developed to be a part of Quality Star, for use in some realms of Swedish psychiatry. The patient is to mark his/her answer to the question “How is your life right now?” on a 100 millimeter long, vertical, visual analog scale. The anchor points of the scale are marked with worst possible life situation and best possible life situation, respectively. A low score signifies a low rating regarding quality of life, while a high score signifies a higher rating for quality of life. In a recent study, the instrument was found to have high reliability and validity (Ivarsson, Malm, Lindström, & Norlander, 2010).
Global Assessment of Functioning (GAF) The GAF (Luborsky, 1962) measures global mental health based on mental, social, and functional capacity. The split-GAF version was used (Pedersen, Hagtvet, & Karterud, 2007) which consists of two scales, one for symptom (GAF Symptom) and one for function (GAF Function). Each scale has 100 steps where score 1 signifies the most severe illness condition, and score 100 signifies that the person is completely free from functional impairment or symptoms (American Psychiatric Association, 1994). The GAF is a frequently used scale with acceptable psychometric properties that have been documented in several studies (e.g., Patterson & Lee, 1995; Yamauchi, Ono, Baba, & Ikegami, 2001).
Procedure
Currently, the Quality Star network consists of 28 different psychiatric clinics that together administer a growing database including 2,348 registered patients. The network was established in 2000 on a small-scale basis, and by 2002 about 10 clinics had already joined. The participating clinics strive to make Quality Star a recurring routine in their practice where the aim is to let the patient undertake the special test battery at least once a year (conducted in relation to the patient’s date of birth). The primary aim has always been to support and ensure a dialogue regarding the patient’s situation, while other aspects such as compiling data in a database for future analyses have gradually developed. Other characteristic features have been the recurring network meetings, directed by the Joint Implementing Group [in Swedish: Gemensamma Genomförande Gruppen, GGG] and the educational material such as practice materials that enable doctors, nurses, or case managers to practice how to rate and calibrate ratings in order to establish a common and comparable norm within the network on how to use the test battery.
The normal procedure is that the patient’s main contact person, or case manager, is responsible for filling out the Quality Star form during one or two ordinary appointments. The test results are then entered into a local database after informed consent has been obtained. This includes information that the procedure facilitates not only comparisons between the analyses of the participant in particular, but also enables compilations for care units/clinics, as well as anonymous comparisons among other districts. The information is provided both orally and in writing, and it is specifically stated that participation is voluntary, and that patients have the right to terminate their participation at any time without giving a motive and without it affecting their treatment.
The research plan was evaluated and approved by the Regional Ethical Vetting Board in Uppsala, and we followed the ethical standards of the World Medical Association declaration of Helsinki concerning Ethical Principles of Medical Research Involving Human Subjects.
Design
In order to make comparisons as accurate as possible for the study, the participation criteria were that the only units that could be part of the study were those that had: (a) used Quality Star since 2002, and (b) since then and until year 2008 regularly, for each year, had reported to the central database, as well as (c) had actively participated in the training courses and calibration exercises of the network. Of the 28 clinics, nine fulfilled these criteria. The first year (2002) was considered a breaking-in and test period, thereby providing all units with a joint starting point – which is the reason why the proper study starts at the beginning of 2003.
Since collected data usually do not meet the demands for normal distribution, neither regarding kurtosis nor skewness, nonparametric statistics were chosen for the analyses. Significant correlations (Spearman’s rho) were found between all values collected during the six years for each of the dependent variables. To facilitate the analyses, it was decided to analyze the material through the mean values from three time periods: Period 1 (2003 and 2004), Period 2 (2005 and 2006), and Period 3 (2007 and 2008) as strong correlations for outcome measures (rhos around .70) could be observed at three time periods.
Results
Differences Regarding Time Periods
Concerning differences in scoring between the three periods, analyses showed (Wilcoxon Signed Ranks Test, p < .05) no significant differences between the periods for three of the measures, namely GQL, GAF Function, and GAF Symptom, whereas significant effects existed for ConSat. Results showed that patients were significantly more satisfied with their care during Period 2, as compared to Period 1 (z = 3.75, p < .001) and with Period 3 as compared to Period 2 (z = 3.29, p = .01) and Period 1 (z = 3.12, p = .002). See Table 1 for mean values and standard deviations.
Table 1. Minimum Values, Maximum Values, Means, And Standard Deviations for the Four Measures from Quality Star Over the Three Time Periods (1–3)
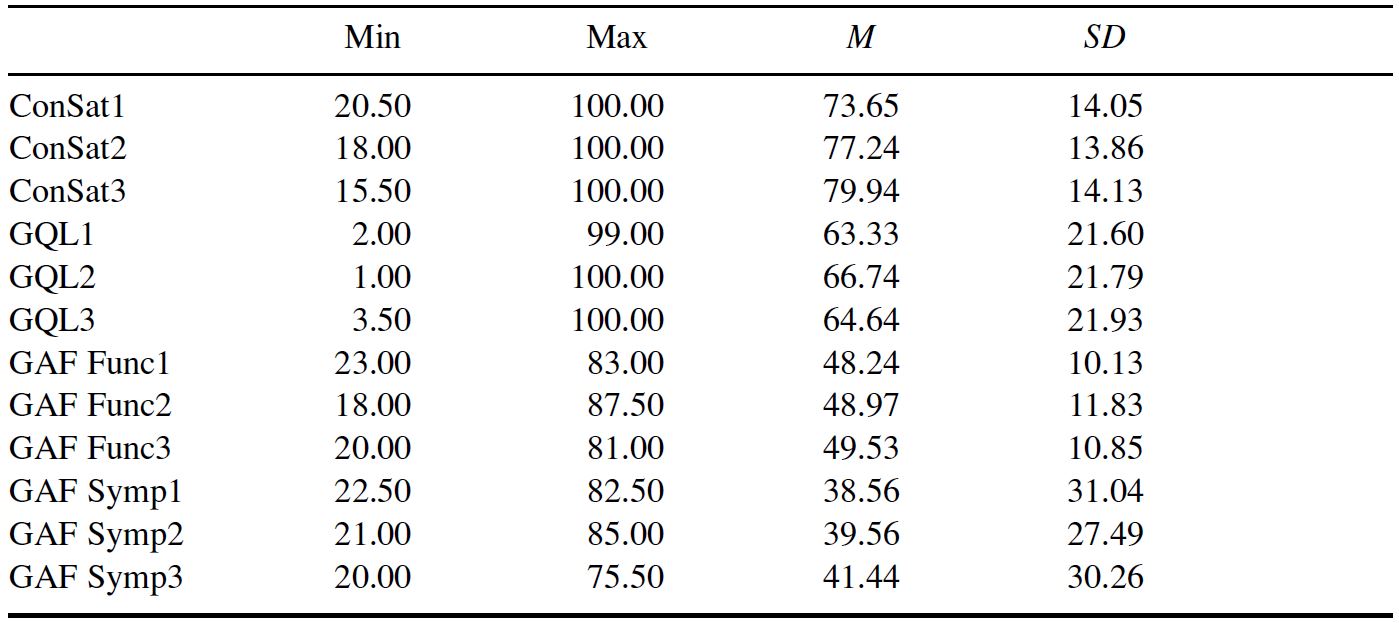
Note: Min = minimum, Max = maximum, M = mean, SD = standard deviation. Quality Star measures = ConSat (consumer satisfaction), GQL (quality of life), GAF Function (psychosocial functioning), GAF Symptom (symptom severity).
Differences Between Patients with Diagnoses Within the Schizophrenia Spectrum or Other Diagnoses
To be able to study differences regarding diagnoses, patients were divided into two groups; those diagnosed within the schizophrenia spectrum (82.8 %, n = 1,139) and those with other diagnoses (17.2%, n = 237). Statistical analyses (Mann-Whitney U test, p < .05) with diagnoses (schizophrenia spectrum, other) as the independent variable and the four measures from Quality Star (i.e., ConSat, GQL, GAF Function, GAF Symptom) from each period (1–3) showed a significant effect for GQL during Period 1, where patients within the schizophrenia spectrum experienced a higher quality of life than patients with other diagnoses (U = 3.17, p < .001). Furthermore, results showed that patients within the schizophrenia spectrum were assessed on GAF Function as having a lower function than patients with other diagnoses for all three periods (U = 3.78, p < .001; U = 4.22, p < .001; U = 2.09, p = .012). Finally, it was shown that patients within the schizophrenia spectrum were assessed on GAF Symptom as having a worse symptom picture than patients with other diagnoses (U = 4.28, p = .002; U = 4.45, p < .001; U = 2.30, p = .012). See Table 2 for mean values and standard deviations.
Table 2. Minimum Values, Maximum Values, Means, and Standard Deviations for the Four Measures from Quality Star Regarding Diagnoses at the Three Time Periods (1–3)
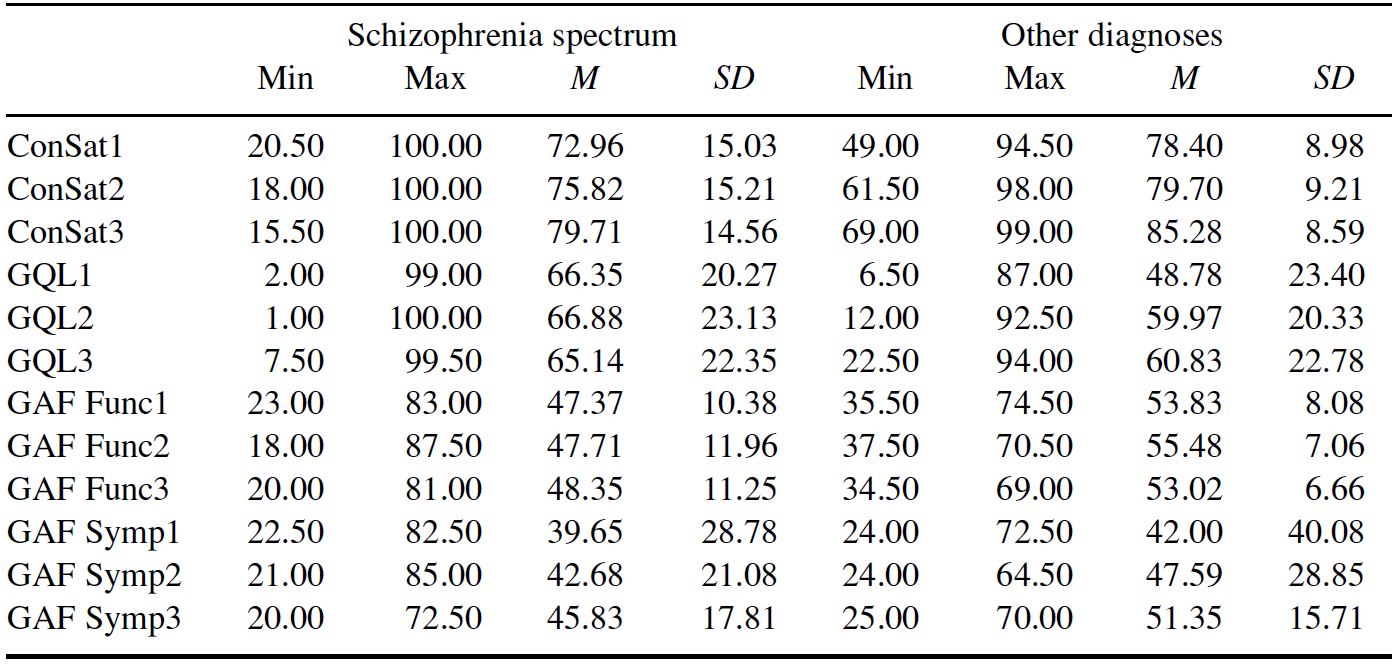
Note: See abbreviations under Table 1.
Differences Regarding Gender
Statistical analyses (Mann-Whitney U test, p < .05) with gender as the independent variable and the four measures from Quality Star (ConSat, GQL, GAF Function, GAF Symptom) from each period (1–3) showed that the women were significantly more satisfied with the care provided (ConSat) during all three periods, than the men (U = 8.46, p = .007; U = 8.70, p = .009; U = 4.11, p = .013). Furthermore, the women had also been assessed on GAF Function as having a better function than the men during Periods 2 and 3 (U = 8.69, p = .041; U = 4.40, p = .044). Post hoc trend tests (within-subjects linear with Bonferroni correction, p < .05) showed that both the women (p = .006) and the men (p = .024) reported increased satisfaction with the provided care for each period, whereas no such significant trends were shown for either gender regarding GAF Function (ps > .05). See Table 3 for mean values and standard deviations.
Table 3. Minimum Values, Maximum Values, Means, and Standard Deviations for the Four Measures from Quality Star Regarding Gender at the Three Time Periods (1–3)
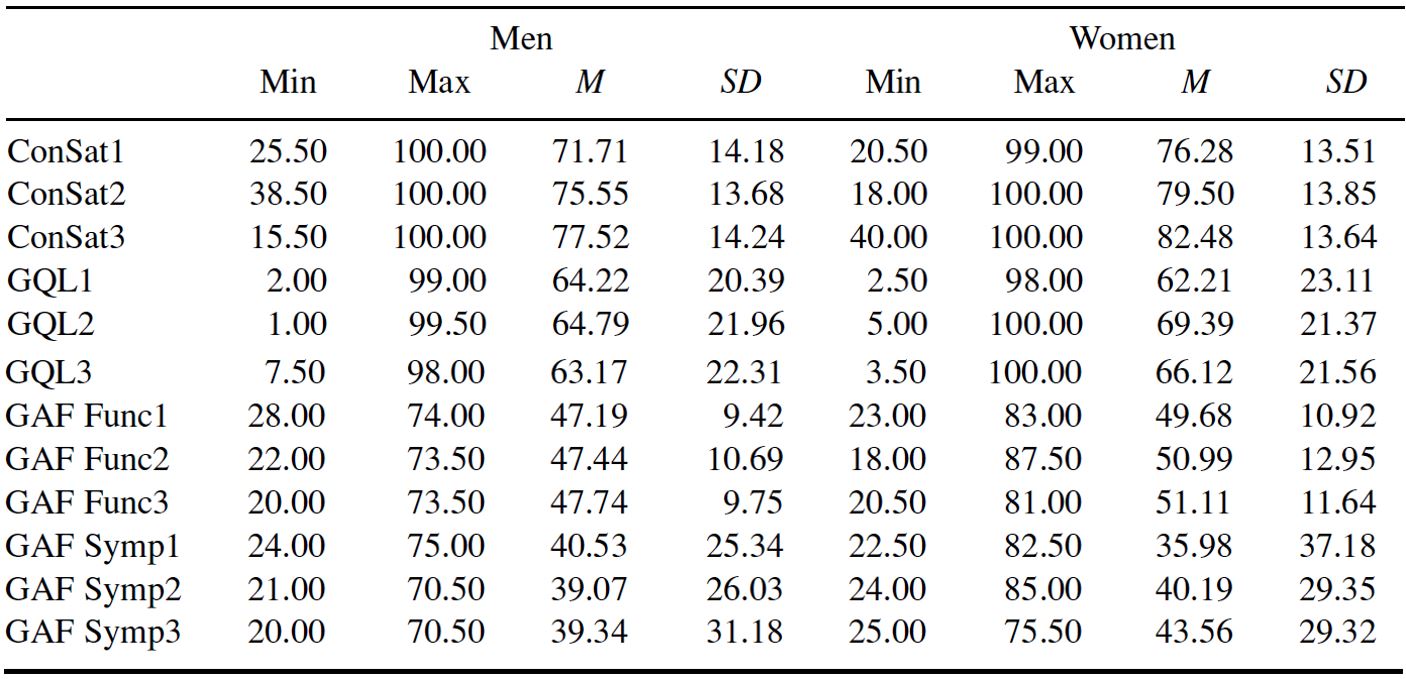
Note: See abbreviations under Table 1.
Differences Regarding Methods of Treatment
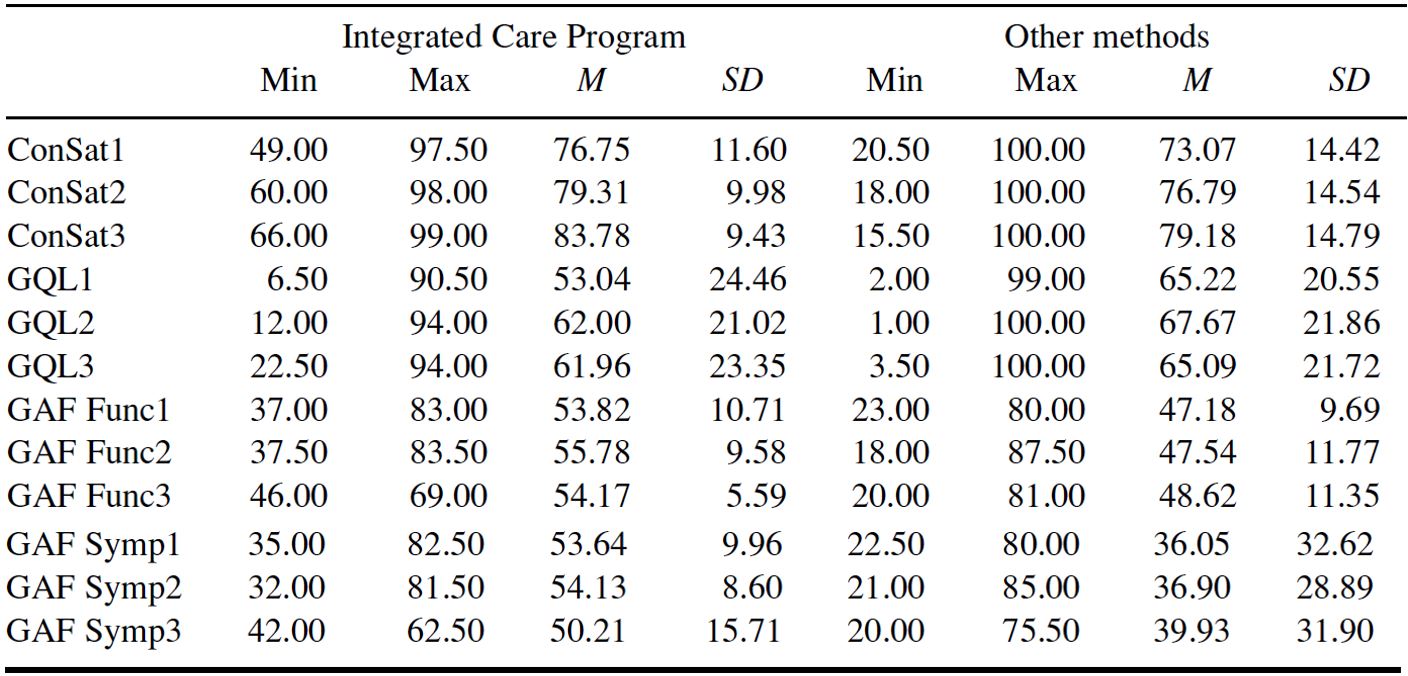
Statistical analyses (Mann-Whitney U test, p < .05) with method (integrated care program, other methods) as the independent variable and with the four measures from Quality Star (ConSat, GQL, GAF Function, GAF Symptom) from each period (1–3) showed that patients at the clinic in Lysekil – who were treated according to the Integrated Care Program method – were assessed as having a better function for all three periods when measured with GAF Function (U = 2.42, p < .001; U = 2.53, p < .001; U = 1.22, p = .004) as well as a better symptom picture when measured with GAF Symptom for all three periods (U = 2.46, p < .001; U = 2.82, p < .001; U = 1.74, p = .044) than the other eight clinics. Results also showed that patients from clinics using other methods experienced a higher quality of life when measured during Period 1 (U = 5.04, p = .006) compared to the clinic in Lysekil. See Table 4 for mean values and standard deviations regarding treatment with the integrated care program or other methods.
Table 4. Minimum Values, Maximum Values, Means, and Standard Deviations for The Four Measures from Quality Star Regarding Method of Treatment at the Three Time Periods (1–3)
Note: See abbreviations under Table 1.
Discussion
The study had two main results: (a) women were more satisfied with the care provided during all three periods than were men, and women were also assessed as having better functioning than men; (b) patients who had undergone treatment according to the integrated care program were assessed as having better functioning (measured with GAF Function) and a better symptom picture (measured with GAF Symptom) for all three periods.
Despite the fact that the Global Assessment of Functioning (GAF) is one of the most widely used instruments within psychiatry, there have been surprisingly few studies with the explicit aim of investigating gender differences. Moreover, the results of the studies that do exist, do not provide a clear-cut picture since some studies indicate that there are gender differences regarding GAF (e.g., Usall et al., 2007; Usall, Haro, Ochoa, Marquez, & Araya, 2002) whereas in other studies no differences were found (e.g., Boggs et al., 2005; Hintikka, Saarinen, Tanskanen, Koivumaa-Honkanen, & Vinamäki, 1999). Research within this area has thus become more focused on finding intermediate variables that explain the different results. One such variable could be that the onset of schizophrenia is earlier for men than for women, which often leads to poorer social functioning in various respects – especially concerning unemployment and housing (Tang et al., 2007; Usall et al., 2007). Other variables of significance as moderators when it comes to gender aspects for the GAF-scale seem to be type of function and depression (Hintikka et al., 1999), symptom pictures, and suicidal tendencies (Tang et al., 2007). Boggs et al. (2005) have shown that the problem with the original GAF scale is that it includes both symptom and function, which has led to the split-GAF (Pedersen et al., 2007) that enables the study of each variable separately. We have not found any previous study in which the split-GAF regarding gender differences has been used, and the result of the current study, which showed that gender differences existed for GAF Function (women had better functioning than men) but not for GAF Symptom, thus needs to be replicated.
Even if both men’s and women’s ConSat scores showed increasing tendencies, the women were significantly more satisfied with the care provided during the entire 6-year period. This result is contrary to that gained in the large-scale EPSILON project, in which the patients’ needs, satisfaction with care, use of service, quality of life, and the health care charges for persons with schizophrenia in five European cities (Amsterdam, Copenhagen, London, Santander, and Verona) were investigated. In a substudy gender differences were investigated regarding satisfaction with care and service (Thornicroft et al., 2002) and no significant differences were found between men and women in this regard. Nor were any gender differences concerning satisfaction with care found in a questionnaire study by the National Committee for Quality Assurance in the USA that included 97,873 men and women who had been patients in the primary health care system (Weisman, Henderson, Schifrin, Romans, & Clancy, 2001). This is, however, not a unanimous picture since in some studies it has been found that women are more satisfied than men with their mental health care (e.g., Röder-Wanner & Priebe, 1995). One explanation for why women express a greater satisfaction in the current study could be the set-up of Quality Star. The studies referred to above only provided a single measuring opportunity whereas Quality Star includes an entire philosophy where the dialogue with the patient is of central importance. It is possible that this communicative aspect is perceived as particularly positive among the female patients.
The Lysekil Clinic has worked with the integrated care program method for more than 15 years (Malmström, 2008). In short, the method, as it has been developed in Sweden, the so-called “Lysekil model”, means that patients with severe problems have their own case managers who coordinate all instances and also provide treatment themselves. The case managers help patients articulate their goals in life and form a resource group. The resource group consists of staff from mental health care, social services, and other instances depending on the needs of individual patients. Relatives or significant others are also included in the resource group. The patients themselves decide who should be part of their resource group, and it is the patients’ goals in life that decide the work of their group. It should also be stated that Quality Star was integrated into the Lysekil model at an early stage, and clinics that, in recent years, have begun working with the integrated care program have also adopted the methods of Quality Star, and vice versa: clinics using Quality Star have joined the network of the Lysekil model. This means that the two networks are growing together more and more, which rules out comparisons between different forms of treatment after 2008 within the framework of this cohort.
Follow-up analyses of the current study demonstrated that the group comparisons conducted on the entire patient group had much the same outcome as the patient group from Lysekil. Concerning diagnoses, however, the differences regarding function and symptom noted for the entire patient group between those within the schizophrenia spectrum and those with other psychiatric diagnoses could not be shown. Whether this excluded difference between the two diagnosis groups among the Lysekil patients is due to the method of treatment or due to something else must be examined for in future studies. Further studies are also needed in order to make comparisons between patients who have undergone traditional examination and treatment, and patients examined with Quality Star and treated according to the integrated care program.
No differences were found concerning results for 3 of the 4 different instruments during different time periods, but it was shown that the patients’ satisfaction with the care increased significantly for each period. That no significant differences were found between the three time periods indicates that the Quality Star can be viewed as a reliable instrument. Every year, new patients are included while others are signed out from their respective mental health care unit or are transferred to other forms of care. That the staff can still maintain a stable level, on average, of the GAF assessments could be an expression that all efforts made in the form of conferences and educational material that give the staff opportunities to calibrate and check how to assess in order to achieve a comparable level, have paid off. More educated, interested, and patient-focused members of staff are likely to lead to improved communication with the patients which, in turn, leads to increased consumer satisfaction (ConSat) with treatment as well as care.
That patients within the schizophrenia spectrum had lower functioning and a poorer symptom picture measured with GAF, than patients with other diagnoses, was an expected result in line with several other studies (e.g., Söderberg & Tungström, 2007; Tungström, Söderberg, & Armelius, 2005) where it has been shown that GAF scores depend on several factors such as diagnoses and psychosocial problems. Patients with diagnoses within the schizophrenia spectrum recurrently have lower GAF scores than a number of other common psychiatric diagnoses (Tungström et al., 2005).
No major significant differences occurred for Global Quality of Life (GQL). This scale could be described as a kind of composite measure that the rest of the Quality Star variables correlate with (Ivarsson et al., 2010). This was also shown in this study where the GQL correlated as calculated with mean values for the whole six year period (Spearman’s rho, ps < .01) with ConSat (.39), GAF Function (.27), and GAF Symptom (.32). Future researchers could investigate which group comparisons the GQL might be of special importance for.
An evidence-based praxis appears self-evident in somatic care. Certainly, the patient with blood pressure problems expects the treating doctor to first measure blood pressure, which is necessary in order for the doctor to know which research-tested interventions ought to be applied. Recurring blood pressure determinations are also necessary for both patient and doctor to later be able to determine whether or not the treatment works. For the same reason, more and more attention is being paid to the fact that it is important for patients and clients within psychiatry and social services to receive evidence-based care (Ivarsson & Malm, 2007; Ivarsson et al., 2010). Test batteries such as Quality Star, in which patients and caregivers cooperate with describing the patient’s whole life situation, could become of great importance for developing an evidence-based practice and accountability within psychiatry.
Ahlfors U. G., Lewander T., Lindström E., Malt U. F., Lublin H., & Malm U. (2001). Assessment of patient satisfaction with psychiatric care. Development and clinical evaluation of a brief consumer satisfaction rating scale (UKU-ConSat). Nordic Journal of Psychiatry, 55, 71-90.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). Washington, DC: Author.
Andersson, J. (2008). Bidrar case management enligt aktivt uppsökande samhällsbaserad behandling och rehabilitering till minskad psykiatrisk slutenvård? [Does case management by assertive community treatment contribute to reduce psychiatric hospitalization?]. Karlstad, Sweden: Karlstad University Press.
Boggs, C. D., Morey, L. C., Skodol, A. E., Shea, M. T., Sanislow, C. A., Grilo, C. M., ... Gunderson, J. G. (2005). Differential impairment as an indicator of sex bias in DSM-IV criteria for four personality disorders. Personality Disorders: Theory, Research, and Treatment, 1, 61-68.
Burns, T., & Firn, M. (2002). Assertive outreach in mental health: A manual for practitioners. Oxford: Oxford University Press.
Eiman G., & Ivarsson, B. (2009). Värden på Kvalitetsstjärnan vid första skattning – relaterat till bakgrundsuppgifter [Perceptions of the Quality Star at first rating – related to background data]. Retrieved December 4, 2009, from http://www.kvalitetsstjarnan.se/Rapporter/SammanfattningAggr2008-10%20v3.pdf
Erdner, L., & Eiman, G. (2003). Jämförande studier mellan Kvalitetsstjärnans anhörigskala och CBS-R-skalan [Comparing the Quality Star Family Burden Scale and the CBS-R scale]. Retrieved December 3, 2009, from http://www.kvalitetsstjarnan.se/Forskning%20studier/Erdner%20Eiman%20dec%202003.pdf
Erdner, L., & Ivarsson, B. (2001). The Quality Star: A tool for regular outcome monitoring. Paper presented at the Second Conference of the European Network for Training, Evaluation and Research in Mental Health (ENTER Mental Health), Paris, October, 2001.
Falloon, I. R. H. (1999). Optimal treatment for psychosis in an international multisite demonstration project. Psychiatric Services, 50, 615-618.
Gemensamma Genomförande Gruppen-gruppen [Joint Implementing Group]. (2009). Global Quality of Life Scale (GQL). Instrument och manual. Ursprunglig svensk version [Instrument and manual. Original Swedish version]. Retrieved December 1, 2009, from http://www.kvalitetsstjarnan.se/Blanketter/SVENSKA/Manual%20PDF.pdf
Hintikka, J., Saarinen, P., Tanskanen, A., Koivumaa-Honkanen, H., & Vinamäki, H. (1999). Gender differences in living skills and global assessment of functioning among outpatients with schizophrenia. Australian and New Zealand Journal of Psychiatry, 33, 226-231.
Ivarsson, B., Erdner, L., & Malm, U. (2006). The Quality Star: An algorithm for the evaluation of mental health services. Presented at the ENMESH conference, Lund, Sweden 10 June 2006. Retrieved December 4, 2009, from http://www.kvalitetsstjarnan.se/Rapporter/THE%20QUALITY%20STAR%20060610.pdf
Ivarsson, B., & Malm, U. (2007). Self-reported consumer satisfaction in mental health services: Validation of a self-rating version of the UKU-Consumer Satisfaction Rating Scale. Nordic Journal of Psychiatry, 61, 194-200.
Ivarsson, B., Malm, U., Lindström, L., & Norlander, T. (2010). The self-assessment Global Quality of Life scale: Reliability and construct validity. International Journal of Psychiatry in Clinical Practice, 14(4), 287-297.
Luborsky, L. (1962). Diagnostic and Statistical Manual of Mental Disorders. Archives of General Psychiatry, 7, 407-417.
Malm, U. (2002). Case management. Lund, Sweden: Studentlitteratur.
Malmström, S. (2008). Brukartillfredställelse: Är det skillnad på brukartillfredställelsen utifrån kön, diagnos och vårdform? [Consumer satisfaction: Are there differences in consumer satisfaction between gender, diagnosis and institutional or non-institutional care?]. Karlstad, Sweden: Karlstad University Press.
Patterson, D. A., & Lee, M. S. (1995). Field trial of the Global Assessment of Functioning Scale – Modified. The American Journal of Psychiatry, 152, 1386-1388
Pedersen, G., Hagtvet, K. A., & Karterud, S. (2007). Generalizability studies of the Global Assessment of Functioning – Split version. Comprehensive Psychiatry, 48, 88-94.
Röder-Wanner, U. U., & Priebe, S. (1995). Schizophrenie und Lebensqualität: Sex spezifische Aspekte [Schizophrenia and quality of life: Sex-specific aspects]. Fortschritte der Neurologie- Psychiatrie [Advances in Neurology and Psychiatry], 63, 393-401.
Söderberg, P., & Tungström, S. (2007). Outcome in psychiatric outpatient services: Reliability, validity and outcome based on routine assessments with the GAF scale. Umeå, Sweden: Print & Media.
Tang, Y. L., Gillespie, C. F., Epstein, M. P., Mao, P. X., Jiang, F., Chen, Q., ... Mitchell, P. B. (2007). Gender differences in 542 Chinese inpatients with schizophrenia. Schizophrenia Research, 97, 88-96.
Thörnborg, U., Nordholm, L., Wallström, Å., & Svantesson, U. (2005). Quality of life assessment for patients with eating disorders. Eating and Weight Disorders, 10, 56-60.
Thornicroft, G., Leese, M., Tansella, M., Howard, L., Toulmin, H., Herran, A., & Schene, A. (2002). Gender differences in living with schizophrenia. A cross-sectional European multi-site study. Schizophrenia Research, 57, 191-200.
Tungström, S., Söderberg, P., & Armelius, B.-Å. (2005). Relationship between the Global Assessment of Functioning and other axes in routine clinical work. Psychiatric Services, 56, 439-443.
Usall, J., Haro, J. M., Araya, S., Moreno, B., Munoz, P. E., Martinez, A., & Salvador, L. (2007). Social functioning in schizophrenia: What is the influence of gender? European Journal of Psychiatry, 21, 199-205.
Usall, J., Haro, J. M., Ochoa, S., Marquez, M., & Araya, S. (2002). Influence of gender on social outcome in schizophrenia. Acta Psychiatrica Scandinavica, 106, 337-342.
Weisman, C. S., Henderson, J. T., Schifrin, E., Romans, M., & Clancy, C. M. (2001). Gender and patient satisfaction in managed care plans: Analysis of the 1999 HEDIS/CAHPS 2.0H adult survey. Women’s Health Issues, 11, 401-415.
Yamauchi, K., Ono, Y., Baba, K., & Ikegami, N. (2001). The actual process of rating the Global Assessment of Functioning Scale. Comprehensive Psychiatry, 42, 403-409.
Figure 1. Graphic presentation of the Quality Star. The recognized abbreviations of the instruments are presented in parentheses. (Taken from Ivarsson, Malm, Lindström, & Norlander, 2010.)
* This axis is intended for group-specific extra measures when suitable. Health screening (SERS) in general is recommended. For psychosis groups, Remission index (RS-S) is now being introduced.
Table 1. Minimum Values, Maximum Values, Means, And Standard Deviations for the Four Measures from Quality Star Over the Three Time Periods (1–3)
Note: Min = minimum, Max = maximum, M = mean, SD = standard deviation. Quality Star measures = ConSat (consumer satisfaction), GQL (quality of life), GAF Function (psychosocial functioning), GAF Symptom (symptom severity).
Table 2. Minimum Values, Maximum Values, Means, and Standard Deviations for the Four Measures from Quality Star Regarding Diagnoses at the Three Time Periods (1–3)
Note: See abbreviations under Table 1.
Table 3. Minimum Values, Maximum Values, Means, and Standard Deviations for the Four Measures from Quality Star Regarding Gender at the Three Time Periods (1–3)
Note: See abbreviations under Table 1.
Table 4. Minimum Values, Maximum Values, Means, and Standard Deviations for The Four Measures from Quality Star Regarding Method of Treatment at the Three Time Periods (1–3)
Note: See abbreviations under Table 1.
Appreciation is due to anonymous reviewers.
Torsten Norlander, Department of Psychology, Karlstad University, SE-651 88 Karlstad, Sweden. Email: [email protected]